The Immunotherapy Revolution
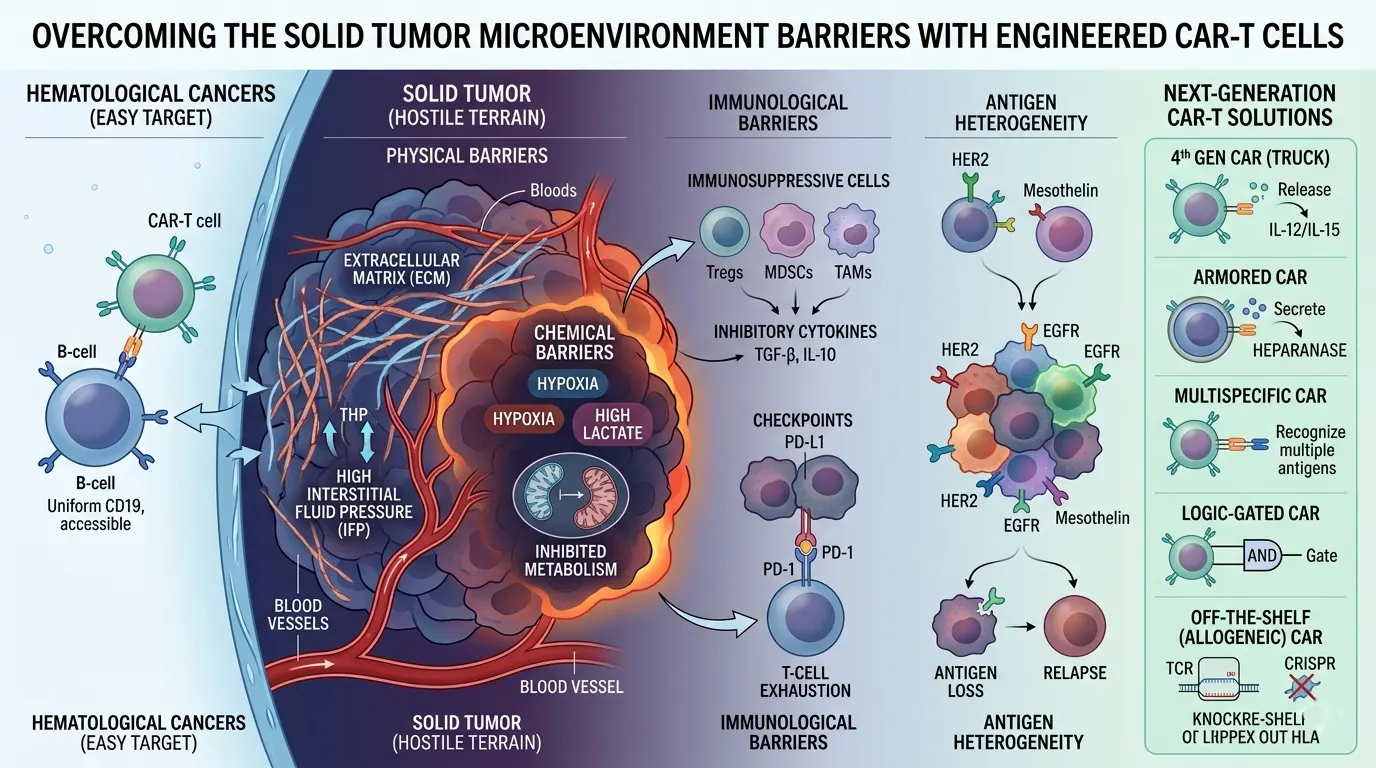
Chimeric Antigen Receptor (CAR) T-cell therapy has redefined the treatment of hematological malignancies, achieving unprecedented durable responses in patients with B-cell acute lymphoblastic leukemia and non-Hodgkin lymphoma. By engineering a patient’s own T-cells to express a receptor that recognizes CD19, we have created a "living drug." However, the application of this technology to solid tumors—such as glioblastoma, pancreatic cancer, and lung adenocarcinoma—has been significantly less successful. For researchers in immuno-oncology, the challenge lies in overcoming the physical, chemical, and immunological barriers of the Solid Tumor Microenvironment (TME).
Molecular Architecture: From First to Fourth Generation CARs
A CAR is a synthetic protein composed of an extracellular single-chain variable fragment (scFv), a spacer/hinge region, a transmembrane domain, and intracellular signaling domains.
1st Generation: Contained only the CD3ζ chain. These cells could recognize tumors but failed to persist or expand in vivo.
2nd and 3rd Generation: Incorporated one or two costimulatory domains (e.g., CD28 or 4-1BB). This was the breakthrough that allowed for sustained anti-tumor activity.
4th Generation (TRUCKs): Also known as "T-cells redirected for universal cytokine killing," these cells are engineered to secrete cytokines like IL-12 or IL-15 upon antigen binding. This helps to "warm up" a "cold" tumor by recruiting and activating endogenous immune cells.
The Hostile Terrain: Physical and Chemical Barriers
Solid tumors are not just clumps of cancer cells; they are complex "organs." The physical barrier created by the extracellular matrix (ECM) and high interstitial fluid pressure prevents T-cells from penetrating the tumor core. Furthermore, the chemical composition of the TME is toxic to T-cells. Hypoxia (low oxygen) and high levels of lactate (from aerobic glycolysis, the Warburg effect) inhibit T-cell metabolism and effector function.
To address this, academics are exploring "Armored CARs" that express enzymes like heparanase to degrade the ECM. Additionally, metabolic engineering of CAR-T cells to enhance their ability to utilize alternative fuel sources (such as fatty acids) under hypoxic conditions is a major area of research.
Immunosuppression and Antigen Heterogeneity
Even if a T-cell enters the tumor, it faces an "immunological gauntlet." Regulatory T-cells (Tregs), Myeloid-Derived Suppressor Cells (MDSCs), and Tumor-Associated Macrophages (TAMs) secrete inhibitory cytokines like TGF-β and IL-10. Moreover, the tumor cells themselves express "checkpoint" molecules like PD-L1, which bind to the PD-1 receptor on T-cells and induce "exhaustion."
Another critical issue is antigen heterogeneity. Unlike B-cell leukemias, where every cell expresses CD19, solid tumors are highly diverse. If a CAR-T cell targets a single protein (e.g., HER2), the tumor may lose that antigen over time, leading to relapse. Researchers are now developing "multispecific" CARs (Tandem CARs) that can recognize two or more different antigens simultaneously, or "Logic-Gated" CARs that only activate if both Antigen A AND Antigen B are present, thereby increasing specificity and reducing "off-tumor" toxicity to healthy tissues.
The Future: "Off-the-Shelf" and CRISPR-Enhanced CARs
The current CAR-T process is autologous (patient-specific), which is time-consuming and expensive. The goal of "Universal" or "Allogeneic" CAR-T cells is to use healthy donor cells. This requires using CRISPR-Cas9 to knock out the endogenous T-cell receptor (TCR) to prevent Graft-versus-Host Disease (GvHD) and the HLA molecules to prevent rejection by the patient’s immune system.
Furthermore, we are moving toward "Synthetic Notch" (synNotch) receptors, which allow for a more sophisticated "program" where the first antigen encounter triggers the expression of a second receptor or a therapeutic payload. This level of synthetic control will be essential for safely and effectively treating the most aggressive solid tumors.
References
1. June, C. H., & Sadelain, M. (2018). Chimeric antigen receptor therapy. The New England Journal of Medicine, 379(1), 64-73.
2. Lim, W. A., & June, C. H. (2017). The principles of engineering immune cells to treat cancer. Cell, 168(4), 724-740.
3. Labanieh, L., & Mackall, C. L. (2018). CAR T cells for solid tumors: What can naturally occurring T cells teach us? Cancer Cell, 34(3), 359-361.
4. Newick, K., et al. (2017). CAR T cell therapy for solid tumors. Annual Review of Medicine, 68, 139-152.
5. Eyquem, J., et al. (2017). Targeting a CAR to the TRAC locus with CRISPR/Cas9 enhances tumour rejection. Nature, 543(7643), 113-117.
6. Rafiq, S., Hackett, C. S., & Brentjens, R. J. (2020). Engineering strategies to overcome the current limitations of CAR T-cell therapy. Nature Reviews Clinical Oncology, 17(3), 147-167.
No comments yet. You can leave the first one.